


The Threat of Long COVID Despite Vaccination
Why the vaccinated need early treatment once infected

Updated!
Looks like I had the right idea back in August 2021 based on a recent study from Oxford Health NHS Foundation Trust titled Six-month sequelae of post-vaccination SARS-CoV-2 infection: a retrospective cohort study of 10,024 breakthrough infections:
“On the other hand, previous vaccination does not appear to be protective against several previously documented outcomes of COVID-19 such as long-COVID features, arrhythmia, joint pain, type 2 diabetes, liver disease, sleep disorders, and mood and anxiety disorders. The narrow confidence intervals (related to the high incidence of these outcomes post-COVID) rules out the possibility that these negative findings are merely a result of lack of statistical power.
*Previously posted to LinkedIn (August 2021)
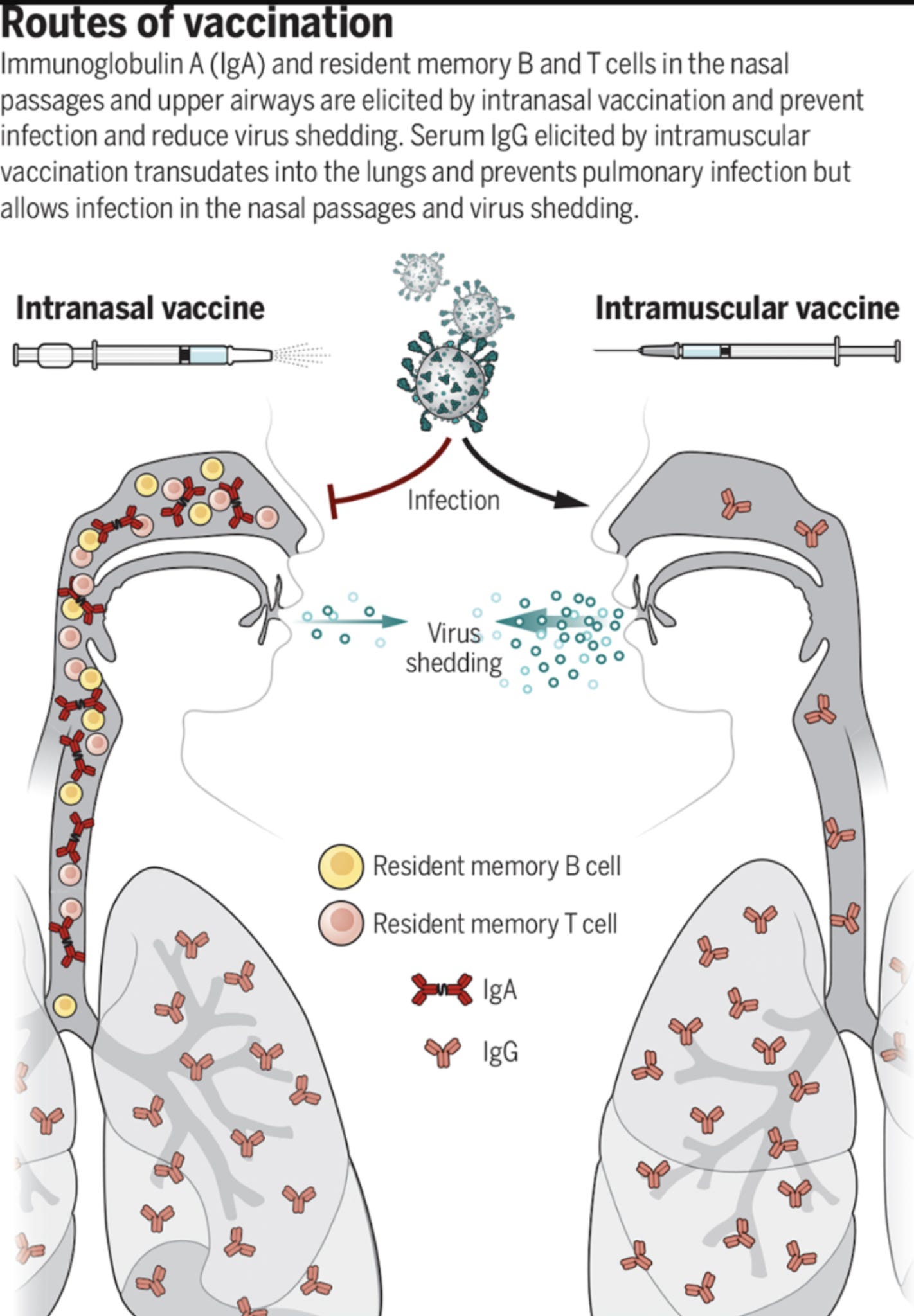
Since I haven't seen anyone broach this topic, I'm going to go on record and say that these current mRNA and adenovirus vector vaccines cannot eliminate the risk of #LongCovid. To understand why, we need to understand the different roles secretory IgA and systemic IgG play in both mucosal and systemic immunity. 👇
"Role of IgA versus IgG in the Control of Influenza Viral Infection in the Murine Respiratory Tract"

Deeper dive into the principles of mucosal immunology👇
"Know your enemy or find your friend?—Induction of IgA at mucosal surfaces”
In a nutshell, these vaccines induce systemic IgG in an effort to protect the lungs. But they cannot arrest the infection and subsequent replication in the upper respiratory mucosa because they do not stimulate durable secretory IgA production.
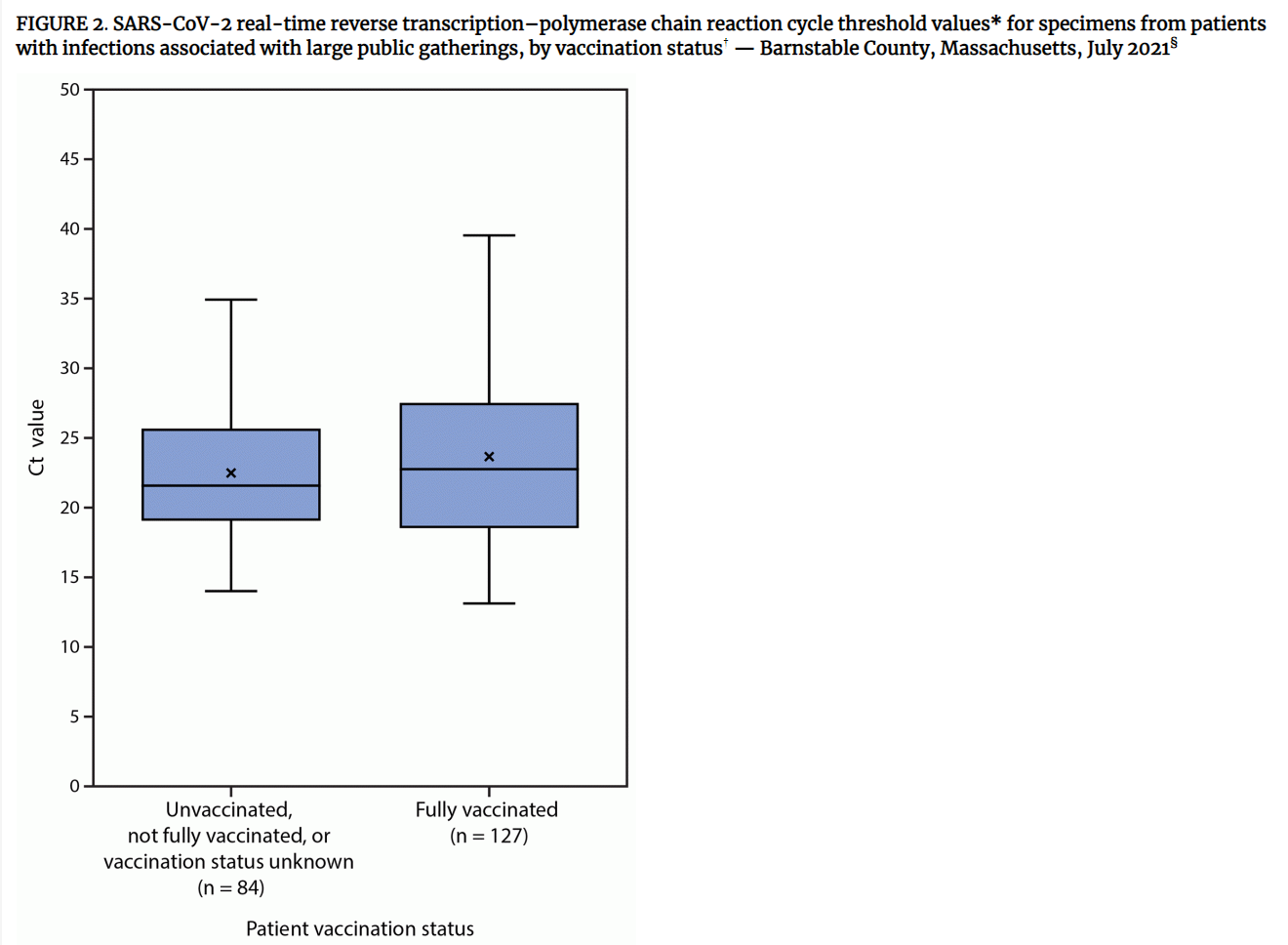
This fact is now easily verified by CDC's recent dive into the Barnstable County, Massachusetts delta outbreak where 74% of the 469 positive infections were fully vaccinated. However, more insightful is the fact that data demonstrated that the viral loads in the vaccinees were often just as high (and higher in some cases) than those of the unvaccinated. *Imperfect estimates by PCR testing*
The consequence of this fact means the virus may replicate and use the olfactory mucosa to enter the CNS irrespective of immediate symptomatology as was demonstrated last year. The problem with that is identified here👇
At this point, it becomes totally obvious that the practice of telling SARS 2 positives to self isolate at home using paracetamol as needed, irrespective of vaccination status, is completely disastrous and constitutes medical malpractice based on established science.
Returning to Long COVID, Patterson et al recently identified critical predictive biomarkers including TNF-alpha, IFN-gamma, IL-6, IL-1α, IL-1β, IL-2, IL-12, CXCL9, CXCL10, VEGF and RANTES that assist in the profiling of long COVID that appears to be driven in large part by persistent non-classical CD16+ monocytes carrying S1 using the fractalkine (CX3CL1)-fractalkine receptor (CX3CR1) activating chronic inflammatory conditions likely via NF-kB transcription factor.👇
The fact that mis-polarized monocytes are carrying S1 instead of self destructing (apoptosis) means that these current vaccines will likely exacerbate long COVID symptomatology because the vaccines instruct transfected cells that take up the lipid nanoparticles (Pfizer-BioNTech & Moderna) to manufacture and express the S glycoprotein. The fact that Long COVID patients - who test negative for SARS 2 nucleocapsid protein (ergo, they've never been infected) - treated by Patterson also present these non classical monocytes containing S1 means that the S1 subunit is being cleaved from S2, likely by furin, at some point prior to MHC presentation and subsequent neutralization by systemic IgG.

An interesting corollary involving M1 polarized macrophages:
“Following the activation by lipopolysaccharide (LPS) and Th1 cytokines (such as IFN-γ and TNF-α), macrophages are polarized into M1 macrophages and characterized by TLR-2, TLR-4, CD80, CD86, iNOS, and MHC-II surface phenotypes. These cells release various cytokines and chemokines (for example, TNF-α, IL-1α, IL-1β, IL-6, IL-12, CXCL9, and CXCL10) which exert positive feedback on unpolarized macrophages. That is, these factors attract more unpolarized macrophages to M1 state. Key transcription factors, such as NF-kB, STAT1, STAT5, IRF3, and IRF5 have been shown to regulate the expression of M1 genes. It seems that NF-κB and STAT1 are the two major pathways involved in M1 macrophage polarization and result in microbicidal and tumouricidal functions.”
Remember December 2020 when TNF-alpha, IFN gamma, and IL-6 were identified as the three biomarkers most predictive of disease severity?
Ultimately, the discussion of ivermectin prophylaxis vs the vaccines isn't relevant. The vaccinees clearly should be administered ivermectin and possibly anti-inflammatories (colchicine anyone?) immediately upon symptom onset or positive PCR. This may be the only way to tilt the balance of probable outcomes in one's favor in light of rapidly declining serum IgG titers. Binding the alpha/ß1 heterodimer and preventing SARS 2 from using ORF6 and Nup98 from hijacking importin proteins and disabling interferons in infected cells in the upper respiratory epithelium gives the innate immune system (e.g., NK cells) the best opportunity to clear the virus, in the absence of effective mucosal humoral immunity against SARS 2, prior to chemotaxis into more critical tissues.
I deliberately did not address the very real possibility of antibody dependent enhancement or original antigenic sin here.